























النبات

مواضيع عامة في علم النبات
الجذور - السيقان - الأوراق
النباتات الوعائية واللاوعائية
البذور (مغطاة البذور - عاريات البذور)
الطحالب
النباتات الطبية
الحيوان
مواضيع عامة في علم الحيوان
علم التشريح
التنوع الإحيائي
البايلوجيا الخلوية
الأحياء المجهرية
البكتيريا
الفطريات
الطفيليات
الفايروسات
علم الأمراض
الاورام
الامراض الوراثية
الامراض المناعية
الامراض المدارية
اضطرابات الدورة الدموية
مواضيع عامة في علم الامراض
الحشرات
التقانة الإحيائية
مواضيع عامة في التقانة الإحيائية
التقنية الحيوية المكروبية
التقنية الحيوية والميكروبات
الفعاليات الحيوية
وراثة الاحياء المجهرية
تصنيف الاحياء المجهرية
الاحياء المجهرية في الطبيعة
أيض الاجهاد
التقنية الحيوية والبيئة
التقنية الحيوية والطب
التقنية الحيوية والزراعة
التقنية الحيوية والصناعة
التقنية الحيوية والطاقة
البحار والطحالب الصغيرة
عزل البروتين
هندسة الجينات
التقنية الحياتية النانوية
مفاهيم التقنية الحيوية النانوية
التراكيب النانوية والمجاهر المستخدمة في رؤيتها
تصنيع وتخليق المواد النانوية
تطبيقات التقنية النانوية والحيوية النانوية
الرقائق والمتحسسات الحيوية
المصفوفات المجهرية وحاسوب الدنا
اللقاحات
البيئة والتلوث
علم الأجنة
اعضاء التكاثر وتشكل الاعراس
الاخصاب
التشطر
العصيبة وتشكل الجسيدات
تشكل اللواحق الجنينية
تكون المعيدة وظهور الطبقات الجنينية
مقدمة لعلم الاجنة
الأحياء الجزيئي
مواضيع عامة في الاحياء الجزيئي
علم وظائف الأعضاء
الغدد
مواضيع عامة في الغدد
الغدد الصم و هرموناتها
الجسم تحت السريري
الغدة النخامية
الغدة الكظرية
الغدة التناسلية
الغدة الدرقية والجار الدرقية
الغدة البنكرياسية
الغدة الصنوبرية
مواضيع عامة في علم وظائف الاعضاء
الخلية الحيوانية
الجهاز العصبي
أعضاء الحس
الجهاز العضلي
السوائل الجسمية
الجهاز الدوري والليمف
الجهاز التنفسي
الجهاز الهضمي
الجهاز البولي
المضادات الميكروبية
مواضيع عامة في المضادات الميكروبية
مضادات البكتيريا
مضادات الفطريات
مضادات الطفيليات
مضادات الفايروسات
علم الخلية
الوراثة
الأحياء العامة
المناعة
التحليلات المرضية
الكيمياء الحيوية
مواضيع متنوعة أخرى
الانزيمات

Corynebacterium
 المؤلف:
Fritz H. Kayser
المؤلف:
Fritz H. Kayser
 المصدر:
Medical Microbiology -2005
المصدر:
Medical Microbiology -2005
 الجزء والصفحة:
الجزء والصفحة:
 3-3-2016
3-3-2016
 4514
4514




+
-
20
Corynebacterium
Diphtheria bacteria are pleomorphic, club-shaped rod bacteria that often have polar bodies and group in V, Y, or palisade forms. They can be grown on enriched nutrient media. Their pathogenicity derives from diphtheria toxin, which binds to receptors of sensitive cells with the B fragment. Once the binding process is completed, the active A fragment invades the cell. This substance irreversibly blocks translation in the protein biosynthesis chain. The toxin gene is a component of the β prophage. Local and systemic intoxications are differentiated when evaluating the clinical picture. Local infection usually affects the tonsils, on which the diphtherial pseudomembrane develops. Systemic intoxications affect mainly the liver, kidneys, adrenal glands, cardiac muscle, and cranial nerves. Laboratory diagnosis is based on pathogen identification. The most important treatment is antitoxin therapy. Diphtheria occurs only in humans. Thanks to extensive diphtheria toxoid vaccination programs, it is now rare.
Corynebacterium diphtheriae (Diphtheria)
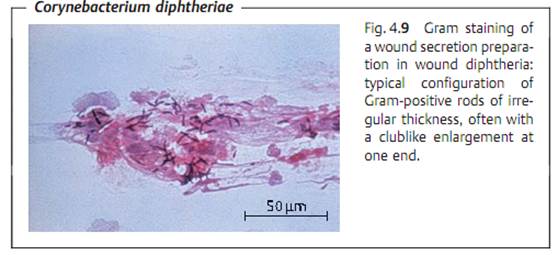
Morphology and culturing. Diphtheria bacteria are Gram-positive, pleomorphic, often club-shaped rods. The individual cells tend to group in V, Y, or palisade arrangements (Fig. 4.9). Neisser staining reveals the polar bodies (polyphosphates stored at one end of the rod).
Loffler nutrient medium, which consists of coagulated serum and nutrient broth, is still used for the primary cultures. Selective indicator mediums containing tellurite are used in selective culturing. K tellurite is used to inhibit the accompanying flora. The K tellurite is also reduced to tellurium, coloring the colonies a brownish black.
Extracellular toxin. Diphtheria toxin consists of two functionally distinct fragments, A and B, whereby B stands for binding to receptors of target cells and A stands for toxic activity. Fragment A irreversibly blocks protein synthesis translation in the target cells, which then die. The toxin gene is always a prophage genome component .
Pathogenesis and Clinical Picture
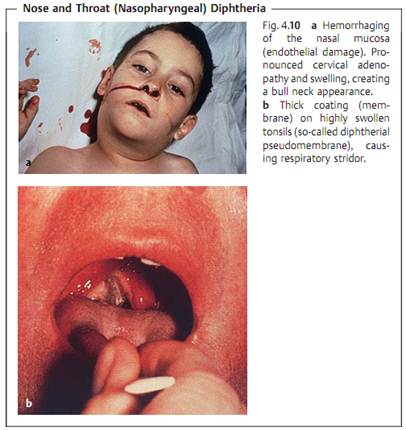
- Local infection. Infection of the mucosa of tonsils, pharynx, nose, and conjunctiva (Fig. 4.10). Wounds and skin lesions can also be infected. The pathogens invade the host through these portals, reproduce, and produce toxin, resulting in local cell damage. The inflammatory reaction leads to collection of a grayish-white exudate, the matrix of the “diphtherial pseudo membrane” consisting of fibrin, dead granulocytes, and necrotic epithelial cells. This coating adheres quite strongly to the mucosa. It may extend into the larynx, thus eventually hindering respiration. Regional lymph nodes are highly swollen.
- Systemic intoxication. Parenchymal degeneration in the cardiac muscle, liver, kidneys, and adrenal glands. Motor cranial nerve paralysis. Late sequel damage due to the intoxication is frequently seen after the acute infection has subsided.
Toxin-negative strains of C. diphtheriae are occasionally observed as pathogens in endocarditis or dermal infections. The pathogenicity of such strains corresponds to that of commensal corynebacteria .
Diagnosis. The method of choice is detection and identification of the pathogen in cultures from local infection foci. The culture smear, which arrives at the laboratory in transport medium, is plated out on Loffler medium and a selective indicator medium. Identification is based on both morphological and physiological characteristics. The toxin is detected by the Elek-Ouchter- lony immunodiffusion test. A molecular method is now also being used to identify the toxin gene. Toxin detection is necessary for a laboratory diagnosis of diphtheria because of the occurrence of toxin-negative strains.
Therapy. Antitoxic serum therapy is the primary treatment and it must commence as soon as possible if diphtheria is suspected. This treatment is supplemented by administration of penicillin or erythromycin.
Epidemiology and prevention. Humans are the sole pathogen reservoir for diphtheria. Infection sources include infected persons and carriers (rare). The disease is usually transmitted by droplet infection, or less frequently indirectly via contaminated objects. The incubation period is two to five days. Incidence levels in central Europe are low. From 1975 to 1984, only 113 cases were reported in Germany. Incidence levels are higher in other countries (Russia). Protective immunization with diphtheria toxoid is the most important preventive measure . Exposure prophylaxis involves isolation of infected persons until two cultures from specimens taken at least 24 hours apart are negative.
 الاكثر قراءة في البكتيريا
الاكثر قراءة في البكتيريا
 اخر الاخبار
اخر الاخبار
اخبار العتبة العباسية المقدسة

الآخبار الصحية


مواضيع ذات صلة
 قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة
قسم الشؤون الفكرية يصدر كتاباً يوثق تاريخ السدانة في العتبة العباسية المقدسة "المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة
"المهمة".. إصدار قصصي يوثّق القصص الفائزة في مسابقة فتوى الدفاع المقدسة للقصة القصيرة (نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)
(نوافذ).. إصدار أدبي يوثق القصص الفائزة في مسابقة الإمام العسكري (عليه السلام)



















