General Aspects of Fungal Disease
Besides fungal allergies (e.g., extrinsic allergic alveolitis) and mycotoxi- coses (aflatoxicosis), fungal infections are by far the most frequent fungal diseases. Mycoses are classified clinically as follows:
Primary mycoses (coccidioidomycosis, histoplasmosis, blastomycoses).-
-Opportunistic mycoses (surface and deep yeast mycoses, aspergillosis, mucormycoses, phaeohyphomycoses, hyalohyphomycoses, cryptococcoses; penicilliosis, pneumocystosis).
-Subcutaneous mycoses (sporotrichosis, chromoblastomycosis, Madura foot (mycetoma).
-Cutaneous mycoses (pityriasis versicolor, dermatomycoses).
Little is known about fungal pathogenicity factors. The natural resistance of the macroorganism to fungal infection is based mainly on effective phagocytosis whereas specific resistance is generally through cellular immunity. Opportunistic mycoses develop mainly in patients with immune deficiencies (e.g., in neutropenia). Laboratory diagnostic methods for fungal infections mostly include microscopy and culturing, in order to detect the pathogens directly, and identification of specific antibodies. Therapeutics for treatment of mycoses include polygenes (above all amphotericin B), azoles (e.g., itraconazole, fluconazole, voriconazole), allylamines, antimetabolites (e.g., 5-flu- orocytosine), and echinocandins (e.g., caspofungin). Antimycotics are often administered in combination.
Fungal Allergies and Fungal Toxicoses
Mycogenic Allergies
The spores of ubiquitous fungi continuously enter the respiratory tract with inspirated air. These spores contain potent allergens to which susceptible individuals may manifest strong hypersensitivity reactions. Depending on the localization of the reaction, it may assume the form of allergic rhinitis, bron chial asthma, or allergic alveolitis. Many of these allergic reactions are certified occupational diseases, i.e., “farmer's lung,” “woodworker's lung,” and other types of extrinsic allergic alveolitis.
Mycotoxicoses
Some fungi produce mycotoxins, the best known of which are the aflatoxins produced by the Aspergillus species. These toxins are ingested with the food stuffs on which the fungi have been growing. Aflatoxin B1 may contribute to primary hepatic carcinoma, a disease observed frequently in Africa and Southeast Asia.
Mycoses
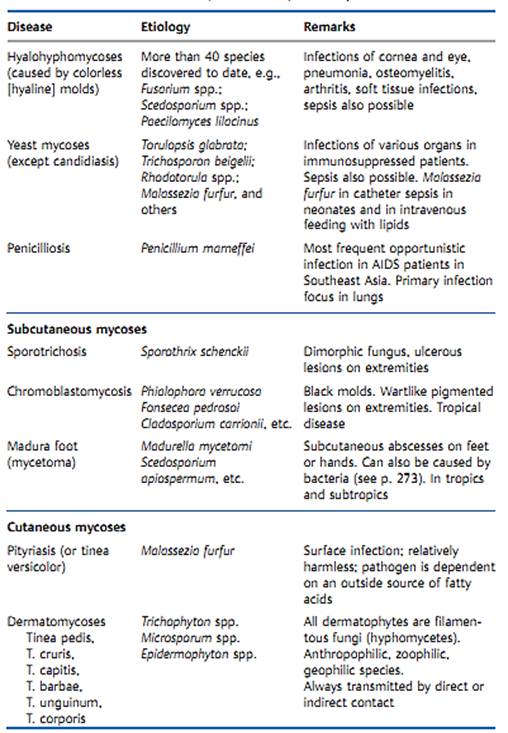
Data on the general incidence of mycotic infections can only be approximate, since there is no requirement that they be reported to the health authorities. It can be assumed that cutaneous mycoses are among the most frequent infections worldwide. Primary and opportunistic mycoses are, on the other hand, relatively rare. Opportunistic mycoses have been on the increase in recent years and decades, reflecting the fact that clinical manifestations are only observed in hosts whose immune disposition allows them to develop. Increasing numbers of patients with immune defects and a high frequency of invasive and aggressive medical therapies are the factors contributing to the increasing significance of mycoses. Table 1 provides a summary view of the most important human mycoses. The categorization of the infections used here disregards taxonomic considerations to concentrate on practical clinical aspects.
Host-pathogen interactions
The factors that determine the onset, clinical picture, severity, and outcome of a mycosis include interactions between fungal pathogenicity factors and host immune defense mechanisms. Compared with the situation in the field of bacteriology, it must be said that we still know little about the underlying causes and mechanisms of fungal pathogenicity.
Humans show high levels of nonspecific resistance to most fungi based on mechanical, humoral, and cellular factors. Among these factors, phagocytosis by neutrophilic granulocytes and macrophages is the most important. Intensive contact with fungi results in the acquisition of spe cific immunity, especially the cellular type. The role of humoral immunity in specific immune defense is secondary.
Table 1 Overview of the Most Important Mycoses in Humans
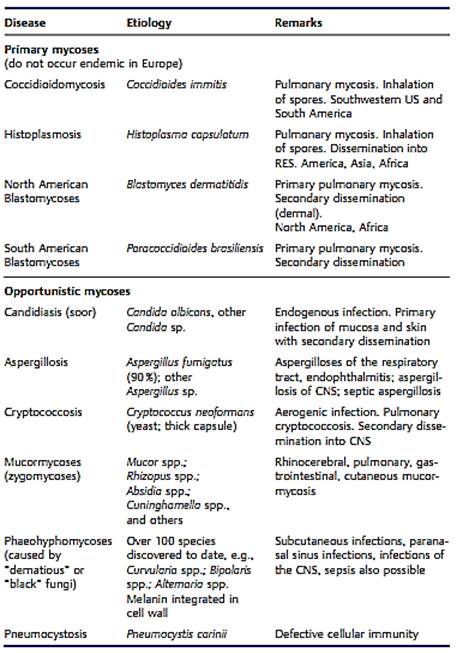
Table 1 Continued: Overview of the Most Important Mycoses in Humans
Diagnosis
The primary concern here is identification of the pathogen
-Microscopy. Native preparation: briefly heat material under coverslip with 10% KOH. Stained preparation: stain with methylene blue, lactophenol blue, periodic acid-Schiff (PAS), ink, etc.
-Culturing. This is possible on universal and selective mediums. Sabouraud dextrose agar can contain selective agents (e.g., chloramphenicol and cycloheximide), this medium has an acid pH of 5.6. The main identifying structures are morphological, in particular the asexual and, if present, sexual reproductive structures. Biochemical tests are used mainly to identify yeasts and are generally not as important in mycology as they are in bacteriology.
-Serology. By the identification of antibodies to special fungal antigens in patient's serum. The Interpretation of serological findings is quite difficult in fungal infections.
-Antigen detection. By finding of specific antigens in the diagnostic material by direct means using known antibodies, possible in some fungal infections (e.g., cryptococcoses).
-Cutaneous test. Cutaneous (allergy) tests with specific fungal antigens can be useful in diagnosing a number of fungal infections.
-Nucleic acid detection. Combined with amplification, such tests are useful for rapid detection of mycotic diseases in immunocompromised patients.
Therapy
A limited number of anti-infective agents are available for specific treatment of fungal infections:
Polyenes. These agents bind to membrane sterols and destroy the membrane structure:
-Amphotericin B. Used In systemic mycoses. Fungicidal activity with frequent side effects. There are conventional galenic form and (new) various lipid forms.
-Nystatin, natamycin. Only for topical use in mucosal mycoses
Azoles. These agents disrupt ergosterol biosynthesis. Their effect is mainly fungistatic with possible gastrointestinal side effects. Hepatic functional parameters should be monitored during therapy:
-Ketoconazole. One of the first azoles. No longer used because of side effects.
-Fluconazole. Oral or intravenous application. For the treatment of surface and systemic mycoses and cryptococcal meningitis in AIDS patients.
-Itraconazole. Oral and intravenous application. Use in systemic and cutaneous mycoses and also for the treatment of aspergillosis.
-Voriconazole. Oral and intravenous application. Good activity against Candida and Aspergillus. No activity against Mucorales.
Antimetabolites. 5-Fluorocytosine. Interferes with DNA synthesis (base analog). Given by oral application in candidiasis, aspergillosis, and cryptococcosis. It is necessary to monitor the course of therapy for the development of resistance. The toxicity of amphotericin B is reduced in combination with 5- fluorocytosine.
Allylamines. Terbinafine. By oral and topical application to treat derma- tomycoses. Inhibition of ergosterol biosynthesis.
Echinocandins.Caspofungin has been approved as a salvage therapy in refractory aspergillosis. It is useful also in oropharyngeal and esophageal candidiasis. Inhibition of the biosynthesis of glucan of the cell wall.
Griseofulvin. This is an older antibiotic used in treatment of dermatomy- coses. By oral application, therapy must often be continued for months
References
Kayser, F. H. (2005). Medical Microbiology. Thieme Stuttgart. New York.





















